Nursing documentation refers to the systematic recording of patient information and care provided by nurses and other healthcare professionals. This documentation is vital for effective communication, continuity of care, legal protection, and quality assurance in healthcare settings. Here are key components and aspects of nursing documentation:
1. Purpose of Nursing Documentation
- Communication: Facilitates seamless communication among healthcare team members.
- Legal Record: Serves as a legal document in case of disputes or audits.
- Patient Care Continuity: Ensures that all healthcare providers have access to the patient’s history and care plans.
- Quality Improvement: Helps in evaluating patient outcomes and improving care practices.
- Research and Education: Contributes data for nursing research and aids in educational purposes.
2. Key Components
- Patient Information: Personal details including name, age, gender, and medical history.
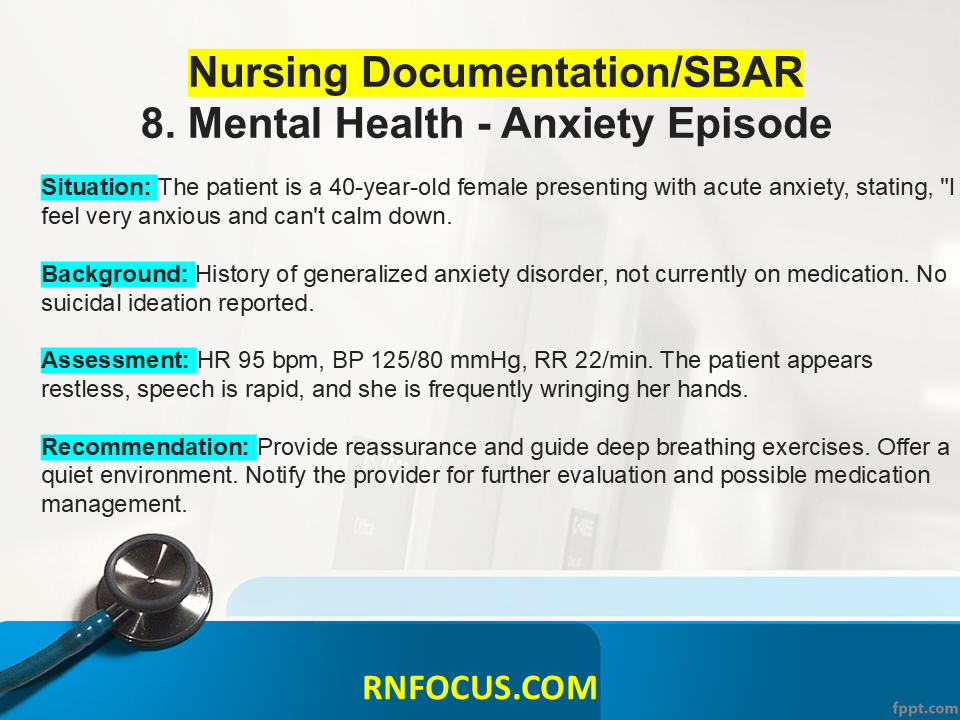
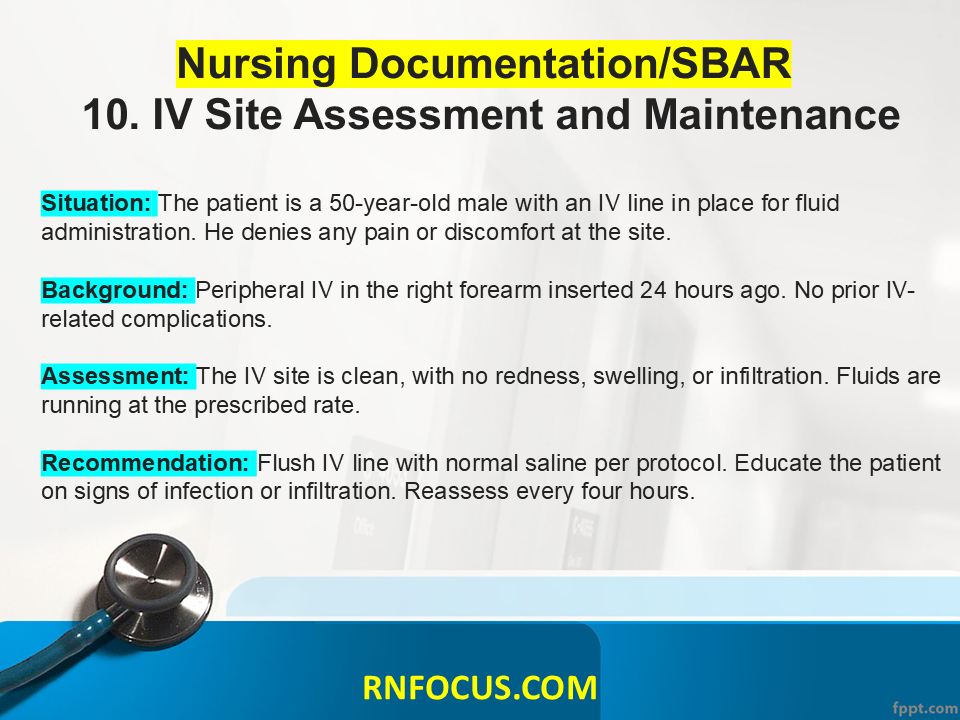
- Assessment Findings: Physical and psychological assessments, vital signs, and any observed signs or symptoms.
- Nursing Diagnoses: Identification of actual or potential health problems based on assessment data.
- Care Plans: Goals, interventions, and expected outcomes tailored to the patient’s needs.
- Implementation Details: Records of the interventions performed, medications administered, and patient education provided.
- Evaluation: Assessment of the effectiveness of interventions and patient responses.
3. Types of Documentation
- Narrative Notes: Detailed, free-text entries summarizing patient care and observations.
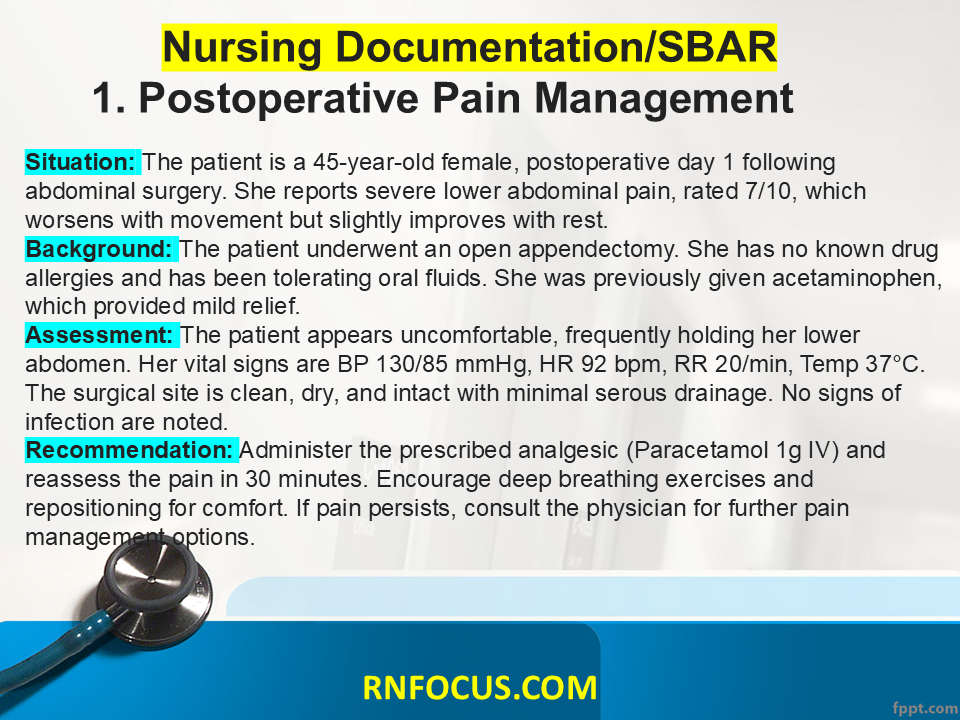
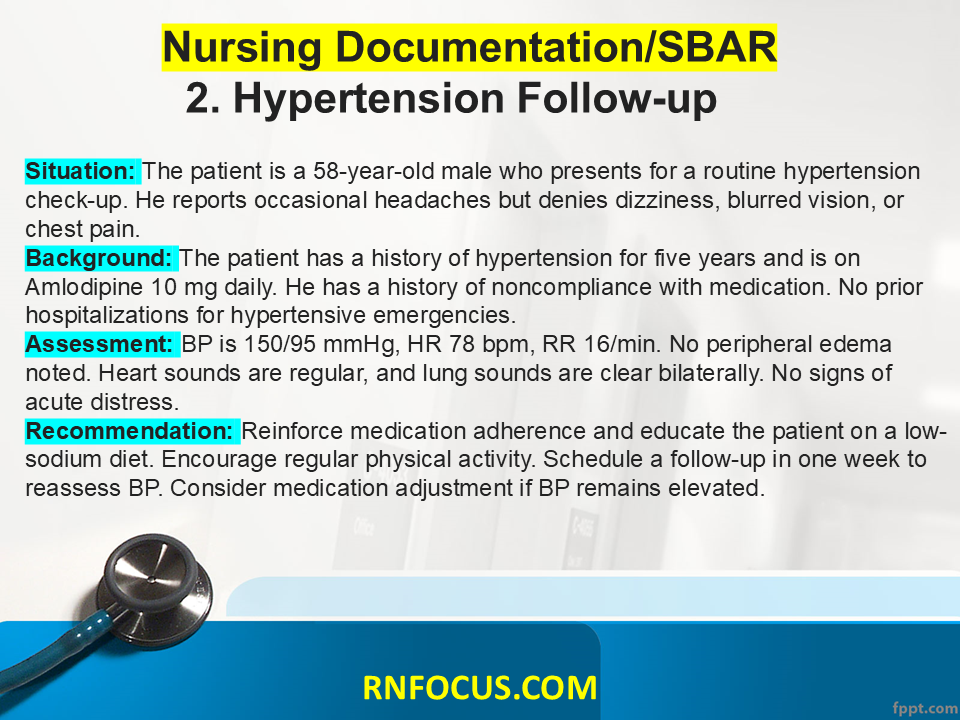
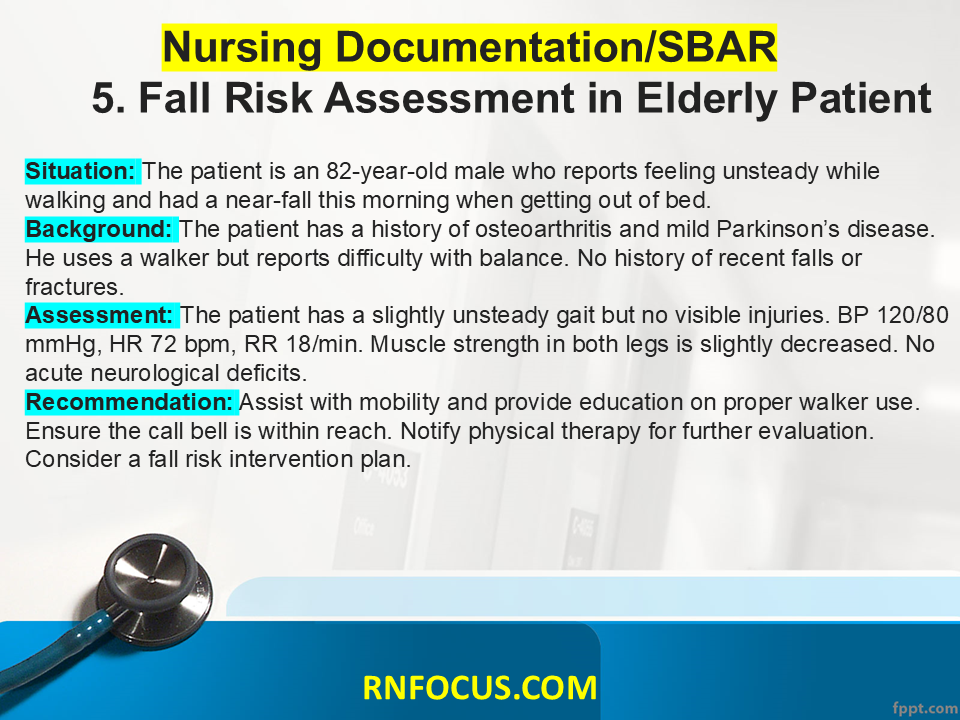
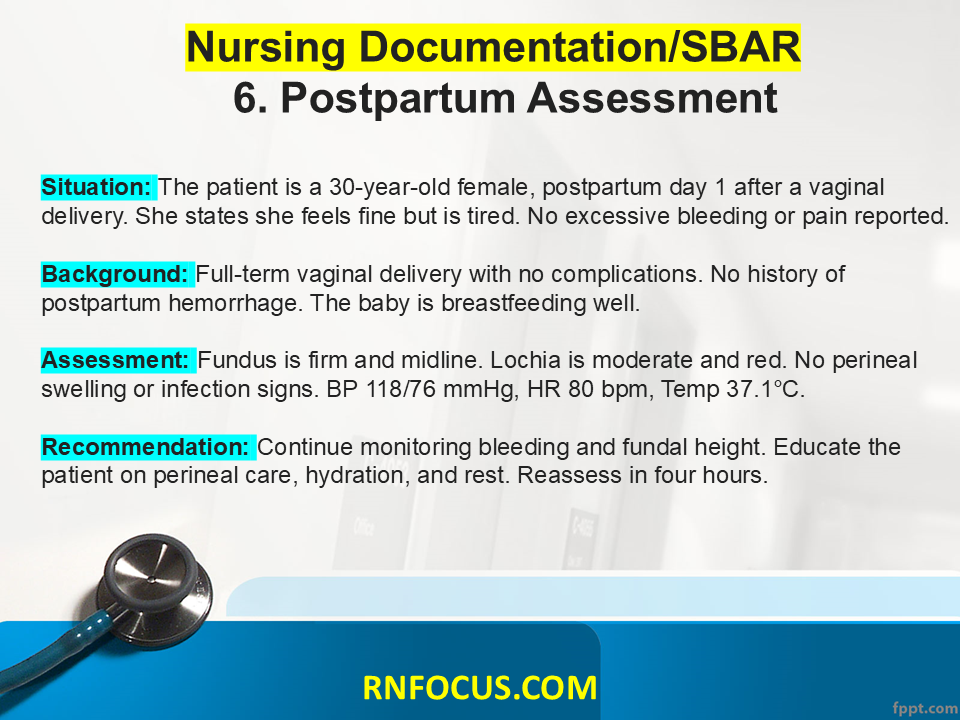
- SOAP Notes: Structured documentation format (Subjective, Objective, Assessment, Plan).
- Standardized Forms: Use of checklists or pre-designed templates for consistency.
- Electronic Health Records (EHR): Digital documentation systems that enhance accessibility and organization.
4. Best Practices
- Accuracy: Ensure all entries are factual, precise, and free from errors.
- Timeliness: Document care and observations promptly to ensure accuracy.
- Confidentiality: Protect patient privacy and adhere to HIPAA regulations.
- Clarity: Use clear and professional language, avoiding jargon and abbreviations that may not be universally understood.
- Consistency: Use standardized language and formats where possible to enhance readability and understanding.
5. Legal and Ethical Considerations
- Always document care as it was provided. Altering or fabricating records can lead to legal ramifications.
- Respect patient confidentiality and only share information with authorized personnel.
- Be aware of mandatory reporting laws for specific situations such as abuse or neglect.
In summary, nursing documentation is an essential aspect of patient care that requires thoroughness, accuracy, and adherence to professional standards. Proper documentation helps ensure high-quality care and facilitates effective communication within the healthcare team.